

As populations age and the burden of non-communicable diseases grows, more families and communities are living with the impact of cognitive decline among older adults. Many are doing so with limited support and services.
At a webinar hosted by the World Health Organization Regional Office for Africa, researchers, clinicians, and care providers came together to examine what dementia means for Africa. While it is often viewed as a condition of old age, experts emphasised that its roots begin much earlier, calling for a shift in how the region understands dementia and responds to it.
Dementia is often mistaken for a normal part of ageing, which can make it easy to overlook in its early stages. In reality, it is not an inevitable part of growing older. It describes a group of conditions that affect memory, thinking, and the ability to carry out everyday activities, with Alzheimer’s and vascular dementia accounting for the majority of cases.
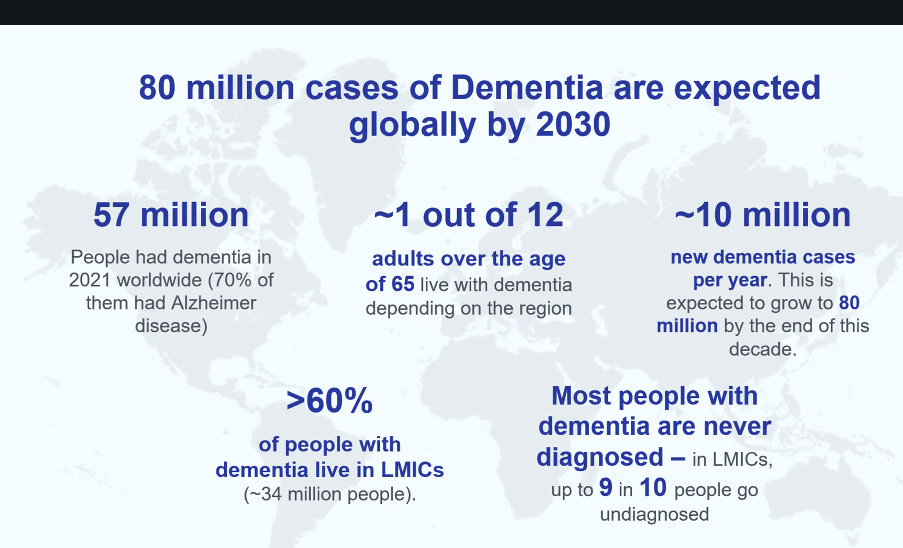
An estimated 57 million people were living with dementia globally in 2021, reflecting a growing but often under-recognised public health challenge. That number is projected to rise to 78 million by 2030 and reach 139 million by 2050, driven by ageing population and shifting disease patterns. More than 60% of cases are in low-and middle-income countries, where health systems are often least equipped to respond and where the gap in available care remains significant.
As this burden continues to grow, there is increasing attention at the global policy level. The political declaration of the fourth high-level meeting of the General Assembly on the prevention and control of noncommunicable diseases and the promotion of mental health and well-being, situates dementia within the broader NCD and mental health agenda, reflecting its growing recognition as a public health priority.
These realities were at the centre of a recent webinar hosted by the World Health Organization Regional Office for Africa, titled “Dementia in the African Region: Strengthening Policy on Integrated Care and Community Support for Older People.”
Dr Rwafa Madzvamutse, Regional Advisor for Mental Health at the World Health Organization Regional Office for Africa, in her presentation drew attention to the multiple and often intersecting factors shaping dementia risk in Africa. Beyond age, factors such as poorly managed HIV, harmful alcohol use, and nutritional deficiencies are increasingly recognised as contributors to cognitive decline.
Dr Madzvamutse also pointed to existing global frameworks, including the WHO Global Action Plan on the Public Health Response to Dementia, Action Plan on the Decade for Healthy Aging and broader mental health and healthy ageing strategies which provide a roadmap for countries to respond. However, it was noted that translating these commitments into practical, context-specific action remains uneven across Africa.
“57 million people worldwide live with dementia. This is as of 2021 we're expecting an exponential increase and that is up to 80 million by the end of the decade. 1 in 12 adults over sixty-five live with dementia, depending on the region. I am looking at the global data and over 60% of people who live with dementia actually live in low-and middle-income countries”
~ Dr Rwafa Madzvamutse
Insights from Nigeria and Kenya
Offering a practical perspective, Ekezie Ralueke Oluchukwu, a dementia care coach and founder of Blue Torch Home Care Ltd, shared how community-based care is being delivered in Nigeria. Founded in 2012, Blue Torch Home Care was established in response to the growing need for home-based support for older adults. Its model centres on integrating family involvement, community engagement, and professional care, recognising that for many people, care happens primarily at home.
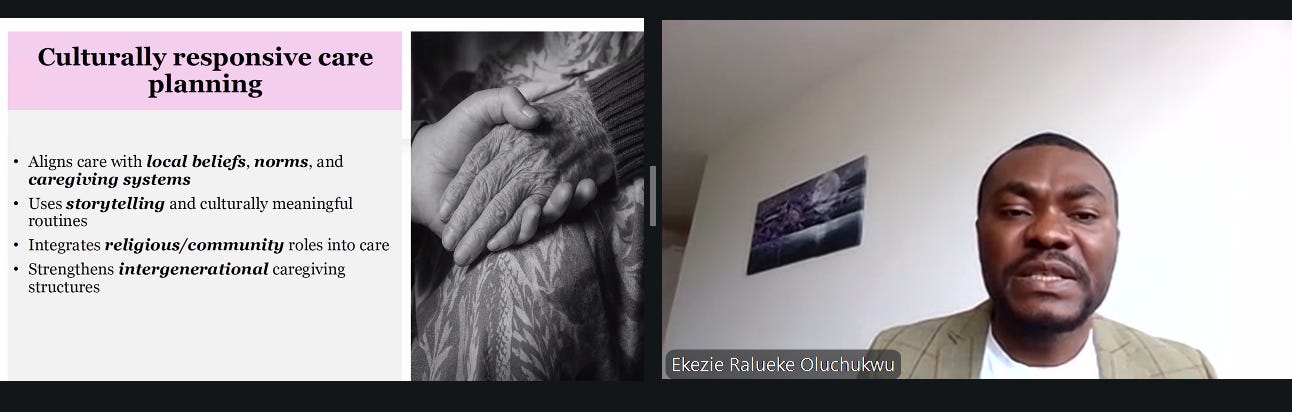
Mr Oluchukwu emphasised that Blue Torch Home Care places strong emphasis on cultural context. Engagement with community leaders, use of familiar social structures, and culturally responsive care practices have helped improve acceptance and uptake of services. In settings where stigma and misconceptions remain, this approach has been critical in opening conversations and encouraging early support. While challenges like late diagnosis, workforce shortages, and financial barriers persist, Blue Torch’s model offers a glimpse of what is possible when care is designed around people’s lived realities and adapted to local contexts.
Additional evidence from rural eastern Uganda also shows how these challenges are unfolding across communities. Presenting findings from a three-year study, Dr Stephen Ojiambo Wandera, a gerontologist, population scientist and a member of the Technical Advisory Group for the UN Decade of Healthy Ageing, highlighted that about 12% of older adults were living with probable dementia, with prevalence increasing significantly with age and disproportionately affecting women.
Beyond age, the data pointed to a convergence of risk factors that are both widespread and, in many cases, preventable. More than half of the older adults studied were socially isolated, while rates of moderate to severe depression were strikingly high. Hypertension was also common, yet many participants were unaware of their status, showing gaps in routine screening and access to care.
In response to these diagnostic and system gaps, tools such as the Informant Dementia Severity Assessment (IDEA) are being used in Uganda, particularly in rural and resource-limited settings.
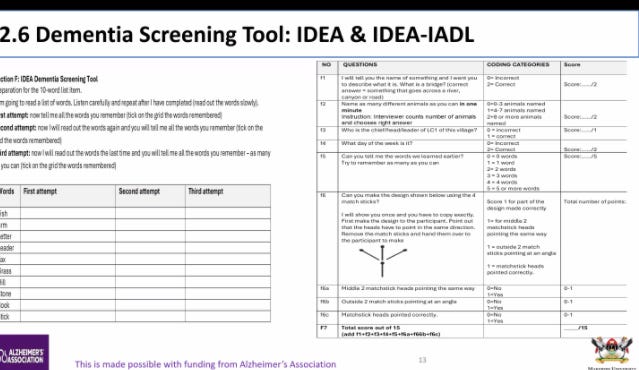
The tool, which assesses domains such as memory, orientation, verbal fluency, and visuospatial ability, is administered in local languages by trained health workers and is used to define cognitive impairment, with studies showing it to be effective in identifying dementia in community settings where low literacy and limited diagnostic capacity remain major challenges.
WHY THIS MATTERS
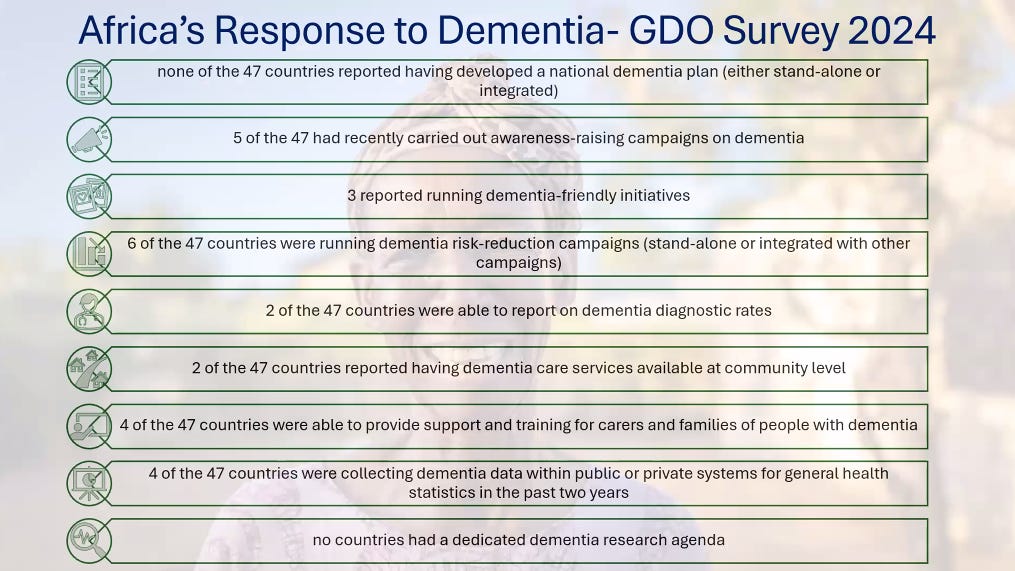
The discussion from the webinar shows that dementia in Africa is a social and systems challenge, beyond being seen as a clinical condition. Data from global policy tracking and the WHO Global Dementia Observatory proves that no African country currently has a fully implemented national dementia plan, with only a few, such as South Africa, Ghana, Kenya, and Ethiopia, having drafts that are yet to be operationalised.
Without a national plan, responses to dementia remain fragmented and underfunded. Care is often informal, falling largely on families and communities rather than being supported through structured health systems. This gap is becoming more concerning as Africa’s population ages and the burden of dementia rises. Projections suggest a sharp increase in the coming decades, which will place further strain on already limited care.